In the last post, we considered how cancer is more than just
one disease. We learned, for
example, that kidney cancer does not necessarily carry the same mutations as
breast cancer. And yet, despite
these variations, certain genes were mutated across several cancer types and
occurred early in the progression of the disease. We called these mutations driver mutations. In
this week’s paper this idea will be reiterated in the context of a new concept:
intratumor heterogeneity: that each
tumor and regions within the same tumor are genetically distinct. The article that prompts this
discussion was published in the New England Journal of Medicine in 2012 (http://www.nejm.org/doi/full/10.1056/NEJMoa1113205).
First: a brief primer on intratumor heterogeneity. Over time, cells acquire genetic
mutations through division errors or external sources that allow them to divide
uncontrollably and operate unchecked.
When these cells start to accumulate, we detect a mass or tumor. Intratumor heterogeneity stems from the
hypothesis that each cancer cell has the capability to acquire different
mutations due to its own genetic instability. As these cells expand and migrate, different tumor cell
regions with distinct genetic profiles exist. Additionally, cells that metastasize or migrate to different
regions of the body can also evolve into different genetic subpopulations. This type of progression is also
referred to as clonal evolution.
To assess if this hypothesis holds true, the authors
analyzed four patients with renal cell carcinoma (kidney cancer), taking
biopsies from multiple tumor and metastatic regions. By sequencing the coding region of the tumor’s DNA and
analyzing the chromosomal copy number, they could identify genetic mutations
and abnormal cell duplication, respectively. For simplicity, we will only discuss Patient 1.
In addition to the renal carcinoma, Patient 1 had metastases
around the kidney area (perinephric), in the lungs and in the chest-wall. From these areas, the investigators
took 15 biopsies including 9 different regions from the primary tumor (See
figure).
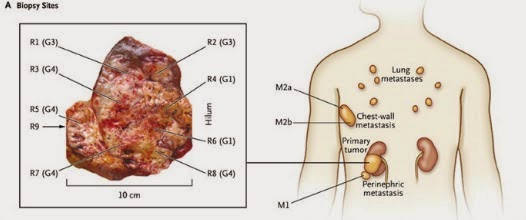
Figure 1 (Gerlinger et al,
NEJM 2012)
After sequencing the tumor material, validating the
mutations, and checking for false positives and/or negatives, the investigators
identified 128 mutations. Of
these, 40 were ubiquitous across every region (only 31%), 59 mutations were
shared between most but not all regions, and 29 mutations, called private
mutations, were present in only one specific region. Excluding the metastatic sites and looking within the tumor
alone, only slightly more mutations were identified as ubiquitously occurring
(34%). The conclusion? Each region
differs slightly at the genetic level.
In addition to
identifying mutations, they analyzed the genetic instability of these tumor
regions. One way to do this is by
assessing the chromosomal copy number.
Normal cells possess two copies and any aberration from this is called
aneuploidy and is a mechanism through which cells can acquire additional
mutations. Ploidy profiling showed
that no region shared the same profile, suggesting that every region – possibly
every cell – has the capability to change and adapt over time and space. The authors referred to this concept as
clonal evolution and suggest that tumors are continually changing, continually
evolving. Like the theory of human
evolution, it is the survival of the fittest. From these results, it becomes clear: intratumor heterogeneity is alive and
well.
Although this seems
like a dire situation, remember that about 30% of regions share the same
mutations. Furthermore, although
the type of mutation was different in different biopsies, several genes were
commonly mutated across several regions.
For example, in Patient 1, these genes were SETD2 and PTEN. They also verified that these genes
were functionally altered showing that their function is important for
maintaining homeostasis. Finally,
the investigators were able to devise a timeline called a phylogenetic tree to
depict where and when some of these mutations occurred. Mutations in specific genes, including VHL, MTOR,
and SETD2 could be considered driver
mutations. And it is these genes
that we need to focus on.
Where do we go from here:
I might call intratumor heterogeneity the silent partner in
cancer research. We acknowledge
its existence but we have yet to figure out what to do about it. Moreover, this silent partner only
points to its parent: the complexity of cancer.
As a researcher this means more focus on identifying and
targeting driver genes. According
to this publication, 30% of mutations are shared. Are these 30 mutations shared
across patients? Moreover, does the clonal evolution of tumors follow a pattern? For example, does a mutation in gene A
lead to a mutation in gene B? This
question probes our ability to predict
gene mutations based on existing mutations. If we can do this, we can design target therapies and
combination therapies that may hit multiple evolutionarily tumor branches and better
fight the disease.
As a patient this study begs for patience: patience at the
clinic where multiple tumor biopsies need to be obtained over multiple time
points. Patience with our
governments as we lobby for more money for these added procedures. And patience with your physician and
the behind-the-scenes researchers who penetrate into the intricacies of your
tumor development, tailoring your treatment.
Today’s uncovered cancer morsel: Just as each of us is
unique, so the tumors that invade our bodies also exhibit singularity.
Gerlinger
M., Rowan A., Horswell S, et al. Intratumor
Heterogeneity and Branched Evolution Revealed by Multiregion Sequencing. NEJM. 2012;366(10):883-892.
No comments:
Post a Comment